Add to wishlist Ajouter au devis Quick view NAME: / CH: / MEDICINE NAME / CH Medication Time / Date Speed Ground flow. primary Lower initials Color: Black/White Quantity: 1000 labels...
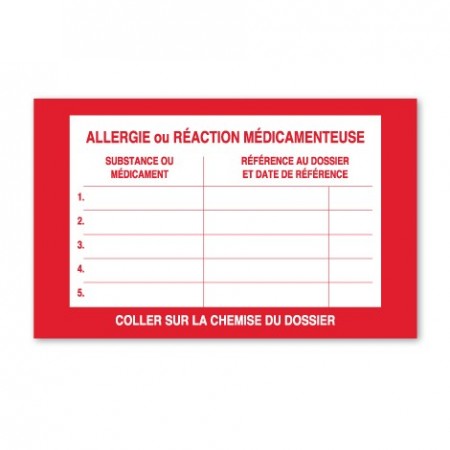
Add to wishlist Ajouter au devis Quick view ALLERGY OR MEDICATION REACTION Allergy or drug reaction (Substance or drug - File reference and reference date) Color: Red/White Quantity: 500 labels per roll...